
Post Contents
BHAGANDAR (FISTULA IN ANO)
Anorectal Fistula
- A fistula is an abnormal communication between two epithelial/endothelial-lined surfaces.
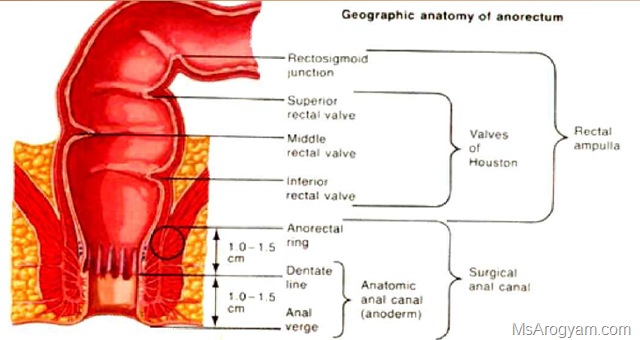
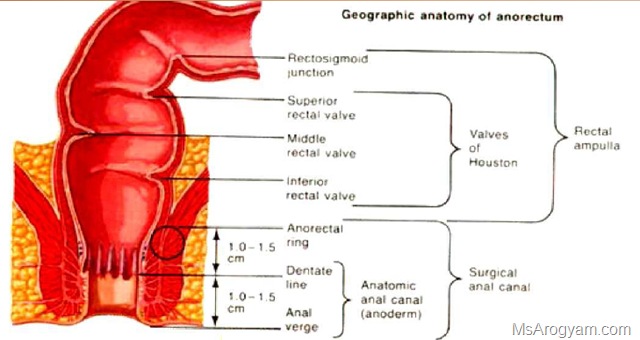
- A fistula in ano has its external opening in the peri anal skin and its internal opening in the anal canal.
Pathophysiology
- Anorectal sepsis can be complicated by a fistula in ano in about 50% of patients during the acute phase of sepsis or within 6 months thereafter.
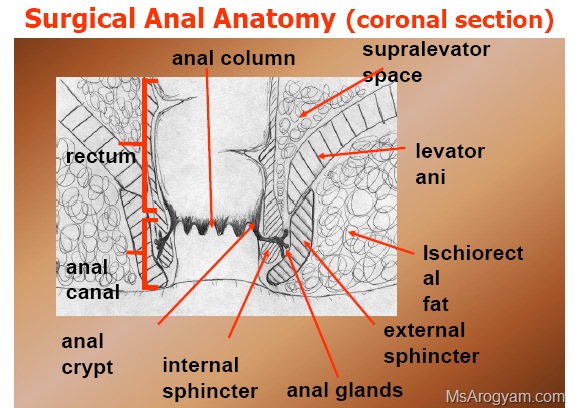
- A fistula in ano forms during the chronic stage of an acute inflammatory process that begins in the intersphincteric anal glands.
- The fistula tracts will follow the course of the original
abscess cavities and subsequent external drainage.
Causative agents
- Escherichia coli 60%
- Staphylococcus aureus 23%
- Streptococcus, B.Proteus 17%
- Always mixed infection
Source of Infection
- Cryptoglandular infection 90%
- Penetration of rectal wall
(bone piece, fish bone or any FB) - Blood borne infection
(TB, Syphillis, AIDS, etc.)
BHAGANDAR (FISTULA IN ANO) Kshar Sutra Treatment
Abscess Anatomy
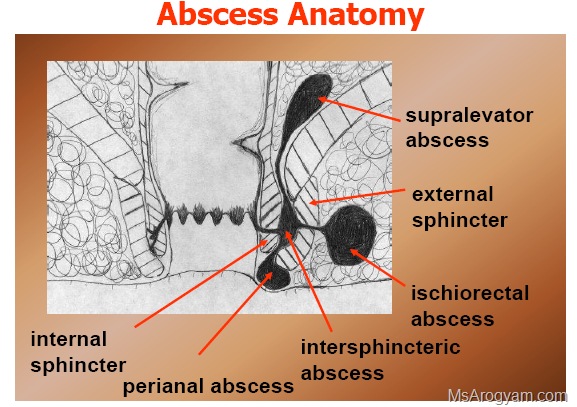
- supralevator abscess, external, perianal abscess, intersphincteric abscess, ischiorectal abscess, internal sphincter
sphincter - An extension from a cutaneus boil
Other cause of FIA
- Crohn’s disease.
- diverticulitis with perforation and fistula to
the perineum; - hydroadinitis suppurativa;
- pilonidal sinus;
- malignancies of the distal rectum, anal
canal or perianal - skin tuberculosis;
- actinomycosis.
Goodsall’s rule
- If the anus is bisected by a line in the frontal plane, an external opening inferior to that line connects to the internal opening via a short direct tract.
- if the external opening is posterior to this imaginary line, the fistula tract follows a curved route to the internal opening in the posterior midline.










Goodsall’s rule Classification of FIA
- Intersphincteric (the most common): The fistula track is confined to the intersphincteric plane.
- Trans-sphincteric: The fistula connects the intersphincteric plane with the ischiorectal fossa by perforating the external sphincter.
- Suprasphincteric: Similar to trans-sphincteric, but the track loops over the external sphincter and perforates the levator ani.
- Extrasphincteric: The track passes from the rectum to perineal skin, completely external to the sphincteric complex. Clinical classification
High anal fistula-
- these open into the anal canal at or above the anorectal ring.
Low anal fistula- - these open into the anal canal blow the anorectal ring.
Sign and symptoms
- Anal fistulae can present with many
different symptoms:-
- Discharge – either bloody or purulent
- Pururitis- itching
- Pain
- Systemic symptoms if abscess becomes infected
Diagnosis
- Diagnosis is by examination, either in an outpatient setting The examination can be an anoscopy.
Possible findings:-
- The opening of the fistula onto the skin may be seen
- The area may be painful on examination
- there may be redness
- An area of induration may be felt – thickening due to chronic infection
- A discharge may be seen
- It may be possible to explore the fistula using a fistula probe (a narrow instrument) and in this way it may be possible to find both openings of the fistula
Digital Rectal examination Better after enema Find
- I. Sphincter tone
- II. Pain or Tenderness
- III. Palpable Mass
- IV. Internal opening of Fistula
- V. Temp
Internal opening of Fistula …… Digital examination
- vi. Male
- Prostate, Seminal vesicles, Base of bladder
- Female
- Uterus, Cervix, Vagina
- Male & Female
- Ischio Rectal Abscess
- Coccyx
Investigations
- Blood- RE
- RBS
- CXR
- Smear C & S
- Fistulogram
Kshar Sutra Chikitsa
Properity of kshar
- Distroys the unhealthy tissues.
- Deberides the wound.
- Promots the healing of healthy tissues.
- It distroys the fibrous tissues and acts as fibrolytic agent.
Materials Required
- I. Lithotomy table within a OT.
- II. Spot light
- III. Ksharsutra dressing trolley
- IV. Instrument box
Preparation of the patient
- Evacuation of bowel
- Shaving of local area
- Inj. T.T.
- Xylocane sensitivity test
- Swedan of local area
- Washing of local area by antiseptic lotion.
Procedure of threading
- • Patient should be keep in lithotomy position.
- • Cleaning by antiseptic lotion and covered by a sterile clothes.
- • Explain the major procedure to patient.
- • Instruct to patient to relax the anal sphincter.
- • Now probing should be done through the path of least resistance under L.A. guided by the finger inside the anal canal.
- • Tip of probe should come out through anal orifice.
- • Now threaded the plain thread of suitable length in the eye of probe. (Primary threading)
- • Pull the probe through the anal orifice to leave the thread behind fistulous track.
- • Now tight the two end of thread moderatly.
- • Finally dressing by Jatyaditail or Anu tail.
- • Chang the thread by kshar sutra at a regular interval of 7 days by rail and train method.
Adjuvent Therapy
- Jatyaditail or anu tail basti
- Sitz bath
- Proper antibiotic
- Haritaki Churn or Panchsakar Churan HS
- Abhayarista 4 TSF BD.
- Analgesics and anti-inflmmatory drugs.
- Diet- nutritious vegetarian diet.
Sitz bath tub
Cut through
- • After subsequent changing of thread, in a few week, ksahar sutra comes out with the knot intact from the tract. This is known as cut through. Cut through indicates complet division of track.
How does Kshar Shutra work!
- • Cutting due to pressure necrossis
- • Kshar helps in cleaning debris from track, sterilization of track
- • Quick and Good healing of track
- • Slow cutting and healing result in nil recurrence and minimal sphincter mechanism distrubances.
-

- Kshar Sutra Treatment In High anal Fistula
-

- Kshar Sutra Treatment In High anal Fistula 2
-

- Kshar Sutra Treatment In High anal Fistula 3
-

- Kshar Sutra Treatment In High anal Fistula4
-

- Kshar Sutra Treatment In High anal Fistula5
-

- Kshar Sutra Treatment In High anal Fistula6
-

- Kshar Sutra Treatment In High anal Fistula7
-

- Kshar Sutra Treatment In High anal Fistula9
-

- Kshar Sutra Treatment In High anal Fistula11

Problem during the therapy
- I. Duration of treatment- depend on the length of track.
- II. Allergic reaction
- III. Discharge
- IV. Incontinence- may be due to trauma to sphincter, so that never cross the ano rectal-ring.
- V. Foreign body sensation.
- VI. Anal stenosis.
Advantage of kshar sutra
- Minimal trauma and no tissue loss as compare to fistulectomy.
- Almost no bleeding as compare to fistulectomy.
- Anesthesia is seldom required.
- Minimal hospital stay.
- No dressing as compare to fistulectomy
- No anal stricture if properly treated.
- Nil recurrence 99.96%
- Very narrow and fine scare as compare to fistulectomy
- Therapy is cost effective.




{kind=link}
i am suffring from fistula in ano since last 2 and half month. May kindly tell me the ayurvedic treatment centres. I am presently in Guwahati. My home town is
delhi.
Go to Government Ayurvedic College, Jalukbari, Guwahati – 781014 & take appointment of Mr. Pankaj Berman
Go to Government Ayurvedic College, Jalukbari, Guwahati – 781014 & take appointment of Mr. Pankaj Berman or Binod kalita…
I have a fisser last 3 month so plz consult me for homeopathy treatment
hello Mr, if you wants the final solution for fissure better use ayurvedic treatment as soon as possible, as if it become chronic fissure which is more painfull and took more time to heal and must treat the cause of it fist.
I am suffering from fistula in ano 2 operations done. but fistula is in the same condition
Hello Mr Joseph, I recommend you Kshar-Sutra for your Fistula as it is the only successful method for fistula treatment without any recurrence , once fistula treated by kshar-sutra it will not develop again.
Dear SIR,
I am taking kshar sutra treatment for ano fistula in bangalore already 7 threadings completed and dr has told me that it requires atleast 25 to 30 thread change
Kindly let me know your comment as I have only one opening near to anal region approximate 4 cm away.
hello Mr Bharatsingh,
as you mentioned that you have already changed the thread 7 times as it seems a bit complicates els if it is just as you mentioned only 4cm away from anal opening it should be healed within 5-9 thread changing, but this can be different from person to person as every bods body react differently to the kshar sutra treatment, and you didn’t mentioned your depth of track as it may be curved or anything els complications so,
for better view you should email your details of treatment with the images to our email id. we will give you genuine advise.
Dear Sir,
Thanks for replying
dr has advised to squeeze and take out pus during daily sitz bath lot ofpus is also coming out.
I will mail the pictutes if you have mail id
Regards
Bharath
How is your condition now? I am also from Bangalore. I need your feedback on Ksharsutra urgently. Are you cured? What is your condition now.
Thanks
dear sir… i am suffring from anal fistula from last 3 year & i have not operated it yet … i have one opening with 3.5 cm after chekup.. it discharge blood & pus after every 7-8 days & feeling heavy pain .. what is the parmanent care for this type of fistula in ano… thanks in advance . .
Hello Mr Raj, Kshar Sutra is only permanent treatment for fistula its success rate is above 99% so go for kshar sutra treatment.
hello sir i facing fistula problem pls suggest me i m so upset nd dipress
pls send me ur contact as well ur hospital details
go to contact page, find all the contact related info emai: info@msarogyam.com ph: +91-9219434343 .
hello i am keshwar i suffring from fistula two and half year i operate it three times last two opration is done by ksharsutra and trac will be out but it is not good it is operated in aiims ..now present times i used hemopathy what i can do..becuse i can use ksharsutra and allopathy surgery..please give me right direction
Hello Mr.Keshwar
as you said you already treated three times, it seems that their must be some puss pockets etc remains , which may cause recurrence of the infection, may be some other causes like immunity weakness etc. as for you i recommend to visit our clinic once then after proper examination i will tell you what is the main reason for recurrence and what can we do for the treatment for it.
mahoday namaskar nainital uttarakhand me kis sthan par ilaaj karaya ja sakta hai? or 1 fistula ke ilaaj ka kitna kharch ho sakta he?
The charges of fistula treatment by Kshar Sutra may varies they depent on the condition of patients situation although it may varies from patient to patients aprox 10k .
Commentsir mai fstula se pidit hu…mai 26 October 2013 ko English surgery krya tha..50 din bit gye abhi tk thik nhi ho paya h jakhm
aaj dr bola ki fir se surgery krna pdega
mai bahut presan hu
mai Gorakhpur u.p me rehta hu
plz meri madad kijiye plzz
Hello mr Dileep, as you have already gone through the surgery, unfortunately in modern surgery the recurrence is verry high it is just make the fistula more complicated and difficult to treat, so as in your case it is better to go for kshar sutra if you wants the final solution of fistula better go for kshar sutra by kshar sutra center.
dear Dr saheb
Ihave complex Fistula in both side and bifurcated like 6 O cloak 7 O cloak and 5 O cloak.please guide how painful is the treatment and how much time consuming and also estimated cost.By the way I am 59 year old having high BP
Hello Mr Binod,
as you already know you have complex fistula it seems a horse shoe shape fistula, yes by kshar sutra it is treatable more effectively then any other process with complete recovery, time will varies according the depth length of the fistula tract as on an average the cutting rate is 1cm /wk , and no problem with bp medicine with the kshar sutra treatment.
hello doc
my problem is that currently m sufferng frm fistula i.e size is 30mm 3 clock as per mri report..near about 22 dayz ago meri kshar sutra ke through surgery hui hai now plz tell me tht thread ko daily rotate karna compulasary hai ya nhi plz help me out
no problem with rotation of kshar sutra, it dosent need to rotate daily it will move by simple daily movements like walking etc.
Dear Dr. Dheeraj,
My Friend is having piles and 3 massa what could be best possible medicine or treatment for the same. He is suffering from it for last some and it comes on on/off basis. Sometimes it bleed because of constipation.
He is getting relief by allopathic treatment but it comes up again and again.
Please suggest with address for treatment. Currently he is in Delhi.
Hello Mr. Manish,as you described that your frnd have 3 piles mass, and dosent have permanent relief from modern treatment, he should go to kshar sutra for permanent treatment, he can visit my clinic its a single day process for piles only after 3-4hr rest he will be discharged and he can go back to delhi, and after that he has to revisit after 7 day just for checkup and further medicine just go to contact us page for contact details etc.
Hi…I am suffering nearly 4 years rectal stricture…I have been several dilation but its not works successfully….is their any treatment in Ayurveda…or any medicine that I can take..it really don’t wont to go surgical…..thnx
hello Mr Myron, as you already have multiple surgery , still i recommend for kshar sutra its not like other modern surgery it will work as in many of my patients of same problem like yours with chronic fissures they are all ok now,
and about medicine you can try our Ms-Pak-B that will help in healing and softening the muscles.
hi where can I by ms pak b….and how can I meet you for my appointment….can you please describe to me your address or any contact number . so I can talk with you briefly…thank you..
Dear sir,
I have been suffering by haemorrhoids for last two years. It occurs
frequently during bowel movement. During bowel movement, round flesh
comes out of anal sphincter. But it is not that big as i have seen in
other patients. It goes back on a gentle push.
Please suggest any kind of treatments for it. Is kshar sutra
appropriate for it? Or its too early to go for surgery as my age is
only of 22.
Please reply me as soon as possible.
Hello ,Dear
as you describe it seems at least Grade-3 Haemorrhoid , so the complete treatment with medicine is quite deficult at this stage,but kshar sutra treatment will remove them permanent once and for all. you dont have to worry just visit our clinic rest leave to us.
I have multiple pilonidal sinuses. not all are infected but one hole discharged some pus and watery substance. Should I go for ksharsutra? Will it be painful? What will be the recovery time?
Hello,
as you have multiple sinuses it will me difficult to say without proper examination just visit any surgeon modern or kshar sutra as it is not a complicated process and kshar sutra is also very easy for sinuses.
respectfully doctor,
this is my father’s MRI FISTULOGRAPHY REPORT.— there is evidence of fistulous tract seen extending from skin of perineum on right side to anal canal.. there is perianal abscess seen on right side.. there is collection seen in presacral space and is extending to right sie along right internal obturator muscle..
and sir there is also an opinion– MRI FINDINGS ARE LINEAR INTERSPHINCTERIC FISTULA WITH PERIANAL ABSCESS AND COLLECTION IN PRESACRAL SPACE AND EXTENDING TO RIGHT SIDE IN PELVIS ALONG RIGHT INTERNAL OBTURAOTR MUSCLE.
PLEASE SIR GIVE ME ADVICE
.. WHAT SHOULD I DO..
Hello Arpit,
as you know your father have high anal fistula and it seems like extending towered horse shoe fistula, for better diagnosis forward the MRI and other reports to my email id info@msarogyam.com
im having fistula since 8 years. i have been taking kshar sutr treatment since 6 months n the fistula is of 3cm.so sir, could u tell me whether it is 100% curable and how long does it take it take to cure completely
6 month for 3 cm is a bit long time, ask your dr what is the problem why it took this much time.
hello docter,
im suffering from fistula in Ano from the past 1 and a half year
Initially docter had diagosed it as peri anal abbcess and they it drained out,but after 2 months , it came back and when i visited the docter,he diagonsed it perianal sinus ,then i had a surgery for it in december 2013,but that surgery wound never get fixed , and discharge remains on.. now recently in the past month (july 2014) i undergo KSHAR SUTRA TREATMENT and most probabily 1 more thread shall be changed to finilaize the treatment as per doc .. now my question is what are the post KSHAR SUTRA treatment care that i should take… i mean should i workout, exercise etc and wat should i restrict in eating ?
REGARDS
sir mera opreton hue 4 din hua hai magar muje bahot dar lagraha hai kyo ki meri age abhi 26 year hai our muje fhisar hua hai jiski vajahse opretion hua hai magar muje sir ye batao ki kitne samay me ye sahi ho jayega our aage koi problem to nahi rahegi na our meri surjary hui hai jisme 3 cm ka chira lagaya hai our usme tanke bhi nahi lagaye hai yah tritment sahi hai our wo kab kitni jaldi sahi ho jayegi our jaldi ricovry laneke liye kya karna padega ans plz hindi me dijiye ga sir muje bahot gabhrahat ho rahim hai
Hello Ritesh ,
your surgery is sphinctrectomy which is just cutting your sphincter muscles to loos the tightness of the anal sphincter which is normal process but it have sometimes complications like incontinence , ksharsutra is preferred over this process due to no complications.
you can’t do anything about it now just wait for the recovery. ans consult the surgeon if any problem occurs .
Hi sir,i have fistula n i m having homeo treat bt no results,wud lyk 2 go for ksharsutra pls tel me is there any pain in the process n hw long it wil take..
Hello Kamaal,
kshar sutra for fistula is different for different patients as the track is differ for each, so the time is varies from 1hr to 2hr as an average and ata our center we uses proper care about pain depend on the patients we use Anesthesia which suits the patients for pain less surgery.
Commentsir.mainefichula ka operation karaya tha pr koi faida nahi hua phir se blood n pas aane laga hai..or mai abhi saudi me hu or mai 1 saal bad india aaunga phir dava karau to koi problem tonahi hai late karne se..ya mai india se dava mangau or khau to kya ye sahi ho jayega… ye fischula hota kis wajah se haiPlease reply.
maine fichula ka operation karayatha pr koi faida nahi hua phir se blood n pas aane laga hai..or mai abhi saudi me hu or mai 1saal bad india aaunga phir dava karau to koi problem tonahi hai late karne se..ya mai india se dava mangau or khau to kya ye sahi ho jayega… ye fischula hota kis wajah se haiPlease reply.
hi sir pichle 20din se latrin ki jagh per 1 funsi hai 2baar fot chuki hai aur 5 din me dobara baan jati hai kiya yeh bhagander ho sakta hai ,aur iska illag medicine khana se ho sakta hai ,or iska kiya treetment hai
sir
I am irritated external piles last six month I have take ayurved treatment 2month but no any improvement does kasharsutra treatment used at home plz send your answer
sir mai do baar anal fistula ka operation karwa chuka hu but doctor ne anal ring ko ko ek taraf se kaat diya hai. aur waha ke upar cheera wala jagah behad sakht ho gaya hai. MATLAB ghaw sukh gaya hai but latrin ki shanka feel hoti rahti hai. aur sabse badi baat sir ghaaw wale butt par kamar ke neeche ke ek jagah se dard shuru hota hai aur pure pair me dard hota rahta hai . yeh dard usi prakar se hai jaise kafi chalne ke baad pairo me dard mahsoos hota hai. sir mai aapke yaha dikhana chahta hu kintu siddharthnagar se hu. aap bataye sir mai kya karu? yaa Gorakhpur ya Banaras me kisi ko sujjest kare…please sir….mai bahut disturb rahta hu…
Initially, I’m diagnosed with Sinus Track in Ano ..after two times of surgery not doctor said it would be Fistula…and suggested to do MRI to decide the next surgery.
Please suggest the right treatment and duration of medication. In general … is the Kshar Sutra more painful process…! Please suggest.
Hello sir, i had a operation for anal polyp and now i m suffering fr anal sprinctor tightness and fissure problem . For which i dont want ay further operation. So can u tell me any alternative treatment or this problem plz?
As for your Fissure and anal sphincter tightness , you can use our Medicinal Pack Ms-Pack-B which will work for you as this pack is best for fissure.
Sir much tym se fresh hoty samay blood air anal Kay rastay main pain hota h kbhi blood aata h kbhi nhi kya yeah piles h
hi dear,
as you feel pain during motions it indicate about fissure and blood may be came from this fissure, if blood come in large amount then it indicates internal piles hemorrhoids.
Dear Sir, I had been treated for fistula by kshar sutra treatment in year 2001, since then I was very fine but from last 7-8 days I am feeling pain at operated area and also have problem in seating on byke. however I am not finding any woond over anus area. please suggest me quick action to be taken.
thank you in advance.
regards.Nadeem
Dear sir mujhe 4 April 2014 se fistula in ano ki problem h, homeopathic, ayurveda ki dava bahut kha chuka hoon, sugar ki problem bhi h, allopathic me surgeon kah rahe hain ki isko operate kara lo, but mujhe post operation se dar lagta hai, kyunki yeh kafi pain full h, kya kshar sutra treatment me ya koi aur treatment me iska ilaz h, aur kya prosser h. Me kab aur kanha treatment le sakta hoon.
Hello Yogesh,
for fistula kshar sutra is best go for proper kshar sutra center , or visit our center.
Sir, I am suffering from fistula in ano since past 2 years. It is 4 cm far fistula at 10’o clock. I would like to go KSHAR SUTRA treatment but I come to know it makes a lot of time to cure. I need to be cure within 40 days ( around 6 Weeks) for some medical test. Is it possible in this treatment or I need to do surgery? Please reply.
Hello Dhanlal , as your fistula is 4cm , and for each cm it took about 1 week so as for your it took 4-5 week.
Hi,
Trans spincentric filtula is developed in my ano. Doctor said 2 surgery are required , one for pus draining , next for main fistula.
In firtst surgery he tied a thread in my ano and the new opening ..
I want to know , is this the normal process..
Please tell me the address and contact details of your’s as I want to go khshar treatment.
Hello Mr Jain.
I cant say what they are trying to do, but in KsharSutra no need for 2nd surgery only one procedure required fro fistula.
Sir I m suffering from fissure..If I go for kshar sutra ten for how many days I have to take bed rest..I m wrkng in central govt..after how many days I will b able to continue my job..
Fistula ka koi pkka ilaj h .jisse ki dubara dubara operation na krvana pde
Kshar sutra is best for fistula in ano, visit my clinic @ muzaffarnagar or @ NOIDA NCR CALL:9219434343
Dear sir my wife is suffering from fistula last one year sir i want to know about female dr. In kanpur who give the treatment of fistula please give the detail of female dr.
I have fistula in ano from last 1 year. Since i never feel pain no bledding stool is coming normal. Now my army medical is near tell me the permanent treatment.